Robots in medicine—it’s not just about Da Vinci surgical systems. The spectrum ranges from handheld drills with optical tracking to laboratory automation systems and exoskeletons for rehabilitation.
This is a hot topic right now: Key patents are expiring, opening the market to new providers. At the same time, AI technologies are enabling entirely new product categories and lowering barriers to market entry. This combination creates a historic window of opportunity for new market entrants.
The downside: Anyone entering this market faces a regulatory landscape that is more complex than that for “traditional” medical devices. As a result, regulatory expertise becomes a decisive competitive advantage.
This article provides guidance.
1. What Robots and Robotic Systems are Used in Medical Technology?
a. Why Robotics is Much More than Just Humanoid Machines
When manufacturers think of “robotics in medicine,” most picture a Da Vinci system: a large robot that controls surgical instruments. The reality is much broader—and many manufacturers do not realize that their product already falls within the realm of robotics.
The spectrum includes at least:
- Surgical assistance systems (ranging from tele-surgery to handheld tools with tracking)
- Rehabilitation and therapy robotics (exoskeletons, gait trainers)
- Laboratory automation systems and pipetting robots (in vitro diagnostics sector)
- Care and service robotics (transport, assistance)
- Prosthetics with actuators (bionic prostheses)
- Autonomous transport systems in hospitals
What all these systems have in common is that they feature sensors, actuators, and software-controlled regulation that physically interacts with the environment based on input data. What distinguishes them is their degree of autonomy—ranging from fully remote-controlled to fully autonomous.
For an in-depth look at autonomous systems in medical technology, see our article on autonomous systems.
b. Three Types of Surgical Robots
The surgical field in particular warrants closer examination, as it exemplifies just how diverse robots can be:
Type 1: Tele-Operation (Master-Slave)
In systems such as the da Vinci from Intuitive Surgical, the control unit and the actuator are completely separate from one another. Surgeons sit at a console and control instruments that operate on the patient—potentially even from another room.
The advantages are significant: The system can scale the surgeons’ “coarse” movements into much finer movements of the instruments. It can filter out the surgeons’ physiological tremor and even compensate for interference from body movements such as the heartbeat.
However, the separation from the surgical site (the so-called “situs”) also has disadvantages: Surgeons cannot see the entire patient. Direct communication with the team—especially the anesthesiologist—is made more difficult. And the system must ensure at all times that the coordinate systems of the console and the surgical site match exactly. A misalignment would pose a serious safety risk.
Type 2: Collaborative Robots (Co-Bots)
With co-bots such as Stryker’s MAKO system, surgeons keep the instrument in their hand while the robot intervenes in their movements—similar to a lane-keeping assist system in a car.
The robot can protect sensitive tissue, keep the surgeons within a defined region, or assist with fine positioning—for example, when drilling an implant site.
Unlike in tele-operation, there is no scaling of the movements here. Instead, the direct connection between the human and the tool is maintained.
A risk we observe in practice: Research institutes often use industrial robots to implement co-bots. However, these are not designed for the kinematics of a surgical setup, often lack inherent safety in their design, and are not optimized for cleaning or for the sterility requirements in the operating room. The leap from research prototype to medical device is therefore particularly significant.
Type 3: Handheld Systems with Tracking
The third type can be compared to a drill equipped with an optical tracking system. Surgeons handle the coarse positioning, while the system performs the fine positioning based on planning data. This is helpful, for example, in retinal surgeries or when milling knee implant sites.
The key difference: The surgeon can intervene fully at any time and withdraw the tool from the surgical field. This offers the highest degree of autonomy—but the assistance with precision is significant.
c. Why Robots Are Becoming Indispensable in Laparoscopy
Today, surgery primarily uses robots in laparoscopy—that is, for minimally invasive procedures in soft tissue. So far, they are less common in neurosurgery or orthopedics.
Why laparoscopy in particular? Because without robotic assistance, it places extreme cognitive demands on the surgical team:
- The translation between hand movement and instrument movement depends on the depth of penetration of the instrument into the body.
- The instrument moves in the opposite direction to the hand movement (lever effect at the access point).
- The camera displays an different orientation.
Surgeons must therefore constantly mentally compensate for three different directional and transmission ratios. Robotic assistance can drastically reduce this cognitive load by automatically compensating for the transmission and enabling intuitive control.
2. Robots: Regulatory Classification Is Crucial
a. Definition of “(Medical) Robot”
a programmed, actuated mechanism with a degree of autonomy that moves within its environment to perform intended tasks. Crucially, a robot always includes a control system.
Source: ISO 8373:2021
In the medical context, IEC 80601-2-77 clarifies the term Robotically Assisted Surgical Equipment (RASE): a medical electrical system that provides powered actuators for manipulating surgical instruments and includes a control system capable of processing and/or generating commands based on sensor information.
Three core elements connect both definitions:
- Actuators that physically interact with the environment
- A programmable control system that controls the actuators
- A degree of autonomy—the system makes at least some decisions independently.
Sensor-based feedback (closed-loop control) is not mandatory in the general definition, but it is the norm in medical practice—and is de facto required by the safety requirements of IEC 80601-2-77 for surgical robots.
Not every active medical device is a robot. An infusion pump has actuators and a control system—but no relevant degree of autonomy. Conversely, not every autonomous system is a robot: AI software that makes diagnoses independently is autonomous but has no actuators.
b. Decision Tree
Not every product with a motor is a robot. But the line is more fluid than many manufacturers think. Ask yourself:
- Does my product have actuators that physically interact with the environment (move, mill, grasp, transport)?
- Does it have sensors that detect the state of the environment (force, position, image, tissue)?
- Is there a software-controlled regulation system that controls the actuators based on sensor data—in other words, a closed-loop control system?
- What is the degree of autonomy? Does the system make decisions independently—even if they are only micro-decisions, such as force limitation?
Anyone who answers “yes” to the first three questions most likely has a robotic system (see Fig. 1). And this changes two things:
- You are at the intersection of several regulatory frameworks simultaneously—including robot-specific standards and other classification pathways (Section 3).
- The specific activities throughout the entire lifecycle differ qualitatively from those of traditional medical devices—from risk management to usability to post-market surveillance (Section 4).
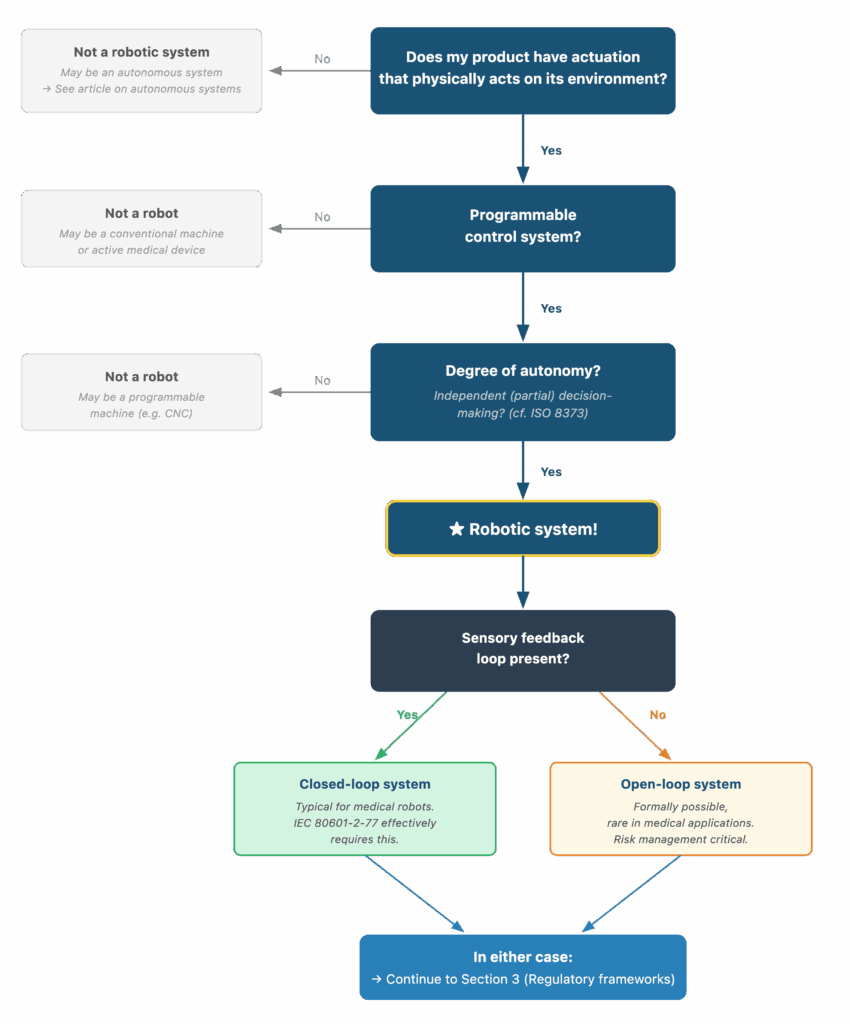
Fig. 1: Three key questions help determine whether a device qualifies as a medical robot (“robotic system”)
3. What regulatory requirements apply?
a. Three regulatory worlds that collide when it comes to robots
What makes robotic medical devices unique from a regulatory perspective is the overlap of multiple regulatory frameworks, each of which is complex in its own right:
MDR (EU) 2017/745 and IVDR (EU) 2017/746
- Every medical device—including robotic ones—must meet the essential safety and performance requirements of the MDR. Classification follows the established rules, with surgical robots typically falling into Class IIb or III due to their invasive nature and active energy emission.
- For laboratory automation systems in the IVD sector, the IVDR applies instead of the MDR—the requirements are structurally very similar, so the regulatory methodology is transferable.
Machinery Regulation (EU) 2023/1230
- Many robots are also machines within the meaning of the Machinery Regulation: They have moving parts that are driven by a power source other than direct human or animal force. This requires an additional risk assessment under the Machinery Regulation and a separate CE conformity assessment.
AI Act (EU) 2024/1689
- As soon as a robotic system contains AI components—whether for image processing, decision support, or autonomous control—the AI Act comes into play. AI-based medical devices in Class IIa or higher are considered high-risk AI systems.
However, the MDR currently takes precedence: Conformity assessment is primarily conducted in accordance with the MDR, while the specific AI Act obligations will take effect at a later date.
b. Robot-Specific Standards
In addition to the “standard” standards for medical devices (IEC 60601-1,
IEC 62304, ISO 14971), there are standards that are specifically relevant to robotic systems:
IEC 80601-2-77 – Surgical Robots
- This specific standard within the IEC 60601 family defines specific safety and performance requirements for RASE (Robotically Assisted Surgical Equipment). Key requirements include, among others:
- Risk management for each degree of freedom of the robot
- Force and speed limits as a protective measure
- Defined stop functions (emergency stop, controlled stop)
- Protection against unintended movement
- Requirements for coordinate system registration between the input and the actuator
The last point is particularly relevant in practice: In tele-operations, the exact alignment of the coordinate systems must be guaranteed at all times—an issue that is not directly addressed in IEC 60601-1 alone.
ISO 13482 – Personal Care Robots
- Defines safety requirements for personal care robots in non-industrial environments, particularly regarding hazards arising from physical contact, autonomy, and navigation.
This standard is expressly not intended for medical applications. However, it can be used as a reference for hazard analysis, particularly for care robots that straddle the line between medical devices and consumer products.
ISO 10218-1/-2 – Industrial Robots
- Safety requirements for industrial robots. Relevant when industrial robot components are incorporated—which is often the case, particularly in co-bot implementations in research. The 2025 revised edition takes collaborative scenarios into account more extensively for the first time.
ISO/TS 15066 – Collaborative Robots
- Defines specific force and pressure limits for human-robot contact. These values are relevant as a starting point for risk assessment, even for medical cobots, but must be adapted for the clinical context (e.g., contact with exposed tissue rather than skin).
IEC 62304 and IEC 62443
- Particularly relevant for robotic systems because they typically contain multiple software systems simultaneously (control, image processing, AI, user interface, safety monitoring) and, due to their interconnectedness and physical impact, are particularly attractive cybersecurity targets.
c. Specifics in Other Markets
FDA (U.S.): Surgical robots in the U.S. are typically cleared via the 510(k) pathway, provided a suitable predicate device exists. For novel systems, the de novo pathway may be considered.
The FDA Guidance on Computational Modeling and Simulation is relevant, although not specific to robots. With robots in particular, the path to a digital twin is short, as these systems are generally described entirely in digital form. Simulation can thus take over parts of the verification and validation process—a significant advantage for systems whose physical test scenarios are complex and expensive.
Other markets such as China (NMPA) and Japan (PMDA) have their own regulatory requirements for medical devices, which also apply to robotic systems.
A detailed examination would go beyond the scope of this article—please contact us if you need support for a specific market.
d. Interim Conclusion: Regulatory Complexity
Given the regulatory complexity, it often makes sense to divide a complete robotic system into several products for regulatory purposes.
- Medical devices
- Accessories
- Non-Medical Devices
This division has a massive impact on effort, costs, and time-to-market—and it determines which standards apply to which components, which conformity assessment procedures must be followed, and whether—and if so, which—authorities or Notified Bodies must be involved.
Ideally, this regulatory strategy should be established at the beginning of every development project—not at the end. This is because it influences not only the approval process but the entire lifecycle: from risk management through clinical evaluation to post-market surveillance. Section 4 shows how this lifecycle for robotic medical devices specifically differs from that of traditional medical devices.
The experts at the Johner Institute specialize in supporting manufacturers of medical devices and IVDs with their regulatory strategy.
4. Differences Between Robotic and “Traditional” Medical Devices?
Anyone familiar with the regulatory landscape (Section 3) knows which requirements apply. The question that is at least as important is: What does this mean in concrete terms for day-to-day development? This is because robotic medical devices differ qualitatively from traditional medical devices throughout their entire life cycle.
a. Risk Management
Risk management in accordance with ISO 14971 applies to every medical device. With robotic systems, however, the risks and risk control measures change:
- Degrees of autonomy create new hazard categories. A system that makes its own (micro)decisions is no longer entirely predictable. This also applies to cobots that “only” intervene in movements.
- AI-specific risks arise when machine learning is used: bias, drift, and opacity in decision-making; in the case of LLMs, additionally: hallucination.
- The coordinate system problem: An error in the alignment between input and actuator is a robot-specific risk that does not exist in any traditional medical device.
- Force, torque, and velocity limits are key protective measures. They must be considered individually for each degree of freedom.
- Multichannel system architectures will likely be necessary—a single autonomous channel is not sufficient for safety-critical decisions. Redundant monitoring is state of the art.
b. State of the Art
An issue that inevitably arises with robotic systems and goes far beyond mere technology: What happens if the robot is potentially better than the state of the art—the human?
In a time-critical situation—such as acute bleeding during surgery—an autonomous system may, under certain circumstances, react faster and more precisely than a human. Must there then be a “human in the loop”—or is it, for safety reasons, precisely not allowed to be there anymore?
As part of the benefit-risk assessment under the MDR, the manufacturer must use the state of the art as a benchmark. If the state of the art is human performance, but the robot surpasses it, a regulatory and ethical gray area arises: The manufacturer must be able to argue why its system is safe enough to act autonomously—or it must justify why it involves a human despite the system’s superior performance. Both require a careful, documented assessment.
c. Usability
The author of this article has researched how surgical robots can provide surgeons with haptic feedback. It is no coincidence that he works in the field of usability engineering at the Johner Institute: In robotic systems, usability and risk management are inextricably linked.
A concrete example: Haptic feedback on a surgical instrument can fulfill two functions simultaneously:
- Information: Inform surgeons about the type of tissue they are interacting with—e.g., whether they are encountering bone
- Control: Actively guide surgeons—e.g., protect sensitive tissue, keep them within a defined surgical region, or help them precisely mill an implant site
The problem: Both functions use the same physical channel—the force/torque feedback on the instrument. If the signals overlap, they can cancel each other out or distort one another. Surgeons then can no longer tell whether the resistance comes from the tissue or from the control assistance.
Haptics has fundamental advantages over visual displays in this regard:
- It acts directly on the hand in three dimensions. Displays remain fundamentally two-dimensional—even with 3D representations. Accordingly, input devices for displays are also mostly two-dimensional.
- Because haptics acts directly within the hand-eye coordinate system, no coordinate transformation by the user is required, as is the case with visual displays.
- Reaction times to haptic/tactile stimuli in humans are shorter than those to visual or auditory stimuli.
This example illustrates why usability testing for robotic systems is qualitatively different from that of traditional medical devices: The interaction has more degrees of freedom, the system’s feedback is more complex, and the system’s behavior—especially at higher levels of autonomy—is less predictable. The user must not only operate the system but also understand when to trust it and when not to.
d. Clinical Evaluation and Testing
How does one clinically evaluate a system that operates semi-autonomously? With robotic systems, the clinical outcome depends even more heavily on the interaction between human and machine than with other medical devices—and this interaction varies depending on the skill of the operating personnel, the configuration, and the clinical context.
Added to this is a practical problem: Clinical trials for surgical robots are usually resource-intensive—while at the same time potentially involving small patient cohorts if the system is intended for niche indications.
This is where the digital twin can offer a real advantage: Because robotic systems are typically described entirely in digital form, simulation can take over parts of the verification and validation process and supplement the clinical evidence.
e. Software
Robotic medical devices typically contain multiple software systems simultaneously: real-time control, image processing, AI algorithms, user interface, and safety monitoring. Each individual system must meet the requirements of IEC 62304—but the real challenge lies in integration and overall behavior.
Particularly critical: the update strategy. If a software update affects the control system, the overall system safety must be reevaluated. With AI components—especially if they come from suppliers—even a single model update can alter the behavior of the entire system.
f. Suppliers
Robotic systems rely on suppliers who must deliver identical components over long periods of time, maintaining consistent quality, meeting required quantities, and ensuring acceptable response times. This applies to mechanical components, sensors, actuators—and increasingly also to AI models, which must be considered supplier components. If a supplier updates its model, the behavior of the entire system may change.
g. Post-Market Surveillance
Market surveillance is becoming more complex due to several factors:
AI Act imposes additional monitoring obligations for AI components. For example, performance drift in autonomous systems in the field must be detected.
Software updates require revalidation of the entire system.
Data collection and analysis must be built into the system architecture from the outset—it is virtually impossible to do so retroactively.Typically, many components must be monitored by third-party manufacturers. This becomes more difficult if these components themselves contain third-party components.
5. Practical Tips for Robotic Medical Devices
a. Proceed in the Correct Order
Anyone entering the field of medical robotics should not skip the following steps—and, above all, should not proceed in the wrong order:
- Classify: Is my product a robotic system? (→ Decision tree from Section 2). This can be easily combined with the next step.
- Define a regulatory strategy: What is my product—or does it consist of multiple products? Not every component has to be a medical device.
- Map the regulatory landscape: Which regulatory frameworks apply? (→ Three worlds from Section 3)
- Identify the standards landscape: Which standards are relevant for my specific product type?
- Establish risk management as an overarching framework: Not as “just one step among many,” but as an overarching structure that guides all subsequent activities
- Only then: Begin development
b. Avoid typical mistakes
Based on our consulting experience, we frequently observe the following patterns among newcomers:
- The Machinery Directive is overlooked. Manufacturers think “medical device = MDR” and forget that a robot can also be a machine.
- The classification path is chosen incorrectly. Especially for systems with multiple components, classification is often performed too late and too broadly.
- Industrial robots are used as the basis for medical co-bots without fully considering the implications for safety, kinematics, and sterility.
- Cybersecurity is addressed too late. In a system that physically interacts with a patient, a security vulnerability has different consequences than it would for an app.
- Clinical evaluation is underestimated. In particular, the question of how to clinically demonstrate the performance of a semi-autonomous system remains unanswered.
- Supplier dependencies are not managed strategically. If the supplier of an actuator module fails, the entire production line comes to a standstill.
- Usability is underestimated. Surgeons do not fully understand exactly what the AI does and does not do. As a result, they may react incorrectly or too late at the decisive moment.
c. Incorporate Post-Market Surveillance from the Very Beginning
A point so important that it deserves its own paragraph: Post-market surveillance for robotic systems is more challenging than for traditional medical devices—and it must be built into the system architecture from the very beginning. Anyone who waits until after the market launch to consider how to collect field data, detect performance drifts, validate and deploy software updates, or minimize risks has a structural problem.
6. Conclusion
Robotic medical devices are more challenging from a regulatory perspective than traditional medical devices—not because the individual requirements are insurmountable, but because multiple regulatory frameworks apply simultaneously and activities throughout the entire lifecycle become more complex.
The good news: Those who understand the regulatory landscape early on and choose a smart strategy can capitalize on current market opportunities.
Contact us—we’ll help you find the right path through the decision tree.